
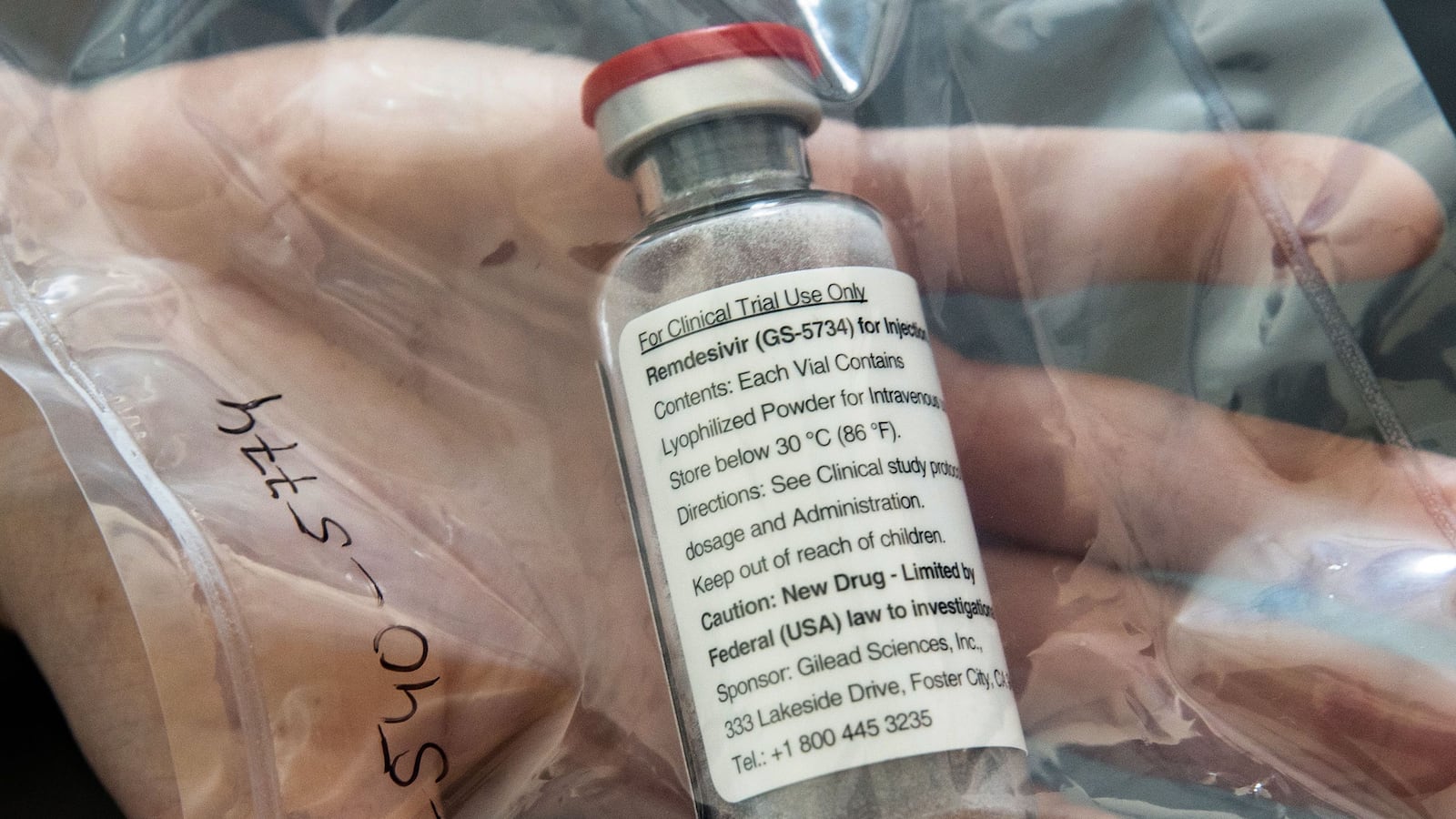
When it comes to treating serious cases of COVID-19, the antiviral drug Remdesivir helps. So do steroids, which can serve to reduce inflammation. And supplemental oxygen, as most Americans familiar with the basics of the coronavirus pandemic might guess, can ease shortness of breath.
The jury’s still out on convalescent plasma, however, despite plenty of hype and U.S. Food and Drug Administration (FDA) controversy. And you shouldn’t count on getting access to experimental monoclonal antibodies like the ones that Donald Trump says got him back out on the campaign trail—at least not anytime soon. Plus, there are a host of once-promising therapies that probably don’t work at all, pointing to the frustratingly short menu of options available to Americans in a slew of states experiencing record COVID-19 hospitalizations.
Welcome to Rabbit Hole, where we dive deep on the biggest story. It’s for Beast Inside members only. Join up today.
With a safe and effective vaccine still weeks or months away under even the best-case scenarios, social distancing and masks remain the best way to prevent COVID, experts stressed.
But if you do catch the disease, a combination of Remdesivir, steroids and supplemental oxygen remains your best hope for recovery, according to front-line physicians canvassed by The Daily Beast.
“There are currently no other treatments that are standard-of-care,” Yogendra Kanthi, a cardiologist at the Northville Health Center in Michigan, told The Daily Beast.
There are caveats, exceptions, and extraordinary circumstances that could weigh on treatment, of course.
“It varies depending on the particulars of a case,” Otto Yang, an expert in infectious diseases at UCLA, told The Daily Beast. “It also varies depending on the institution, although I think most academic institutions have converged on fairly similar principles.”
After declining from a mid-July peak, COVID cases are on the rise again in many U.S. states. There were a record 73,762 new confirmed infections in the United States on Monday, according to Johns Hopkins University’s coronavirus tracker. Alaska, Wyoming, North and South Dakota, Montana, Wisconsin, Tennessee and other states in the Midwest and South are experiencing the greatest rates of increase in new infections in this latest wave.
Chances are most of these infections will be minor. Fewer than 5 percent of COVID cases require hospitalization, according to the U.S. Centers for Disease Control and Prevention. And most hospitalizations don’t result in ventilation.
If you get infected and it’s bad enough to warrant a hospital stay but not so severe that the staff hurries you into intensive care, your doctors are likely to administer Remdesivir to help reduce your viral load, followed by a steroid such as dexamethasone to keep down inflammation. Hits of oxygen can help you through spells of hypoxia.
If that course of treatment sounds familiar, it’s because Trump got Remdesivir, dexamethasone, and supplemental oxygen when he caught COVID himself.
But Trump, who spent just three days at Walter Reed National National Military Medical Center in Maryland before resuming his reelection campaign, also benefited from a cocktail of monoclonal antibodies—an experimental therapy that isn’t available to the vast majority of Americans. The FDA granted Trump a “compassionate use” waiver for the drug from New York pharma Regeneron.
A monoclonal antibody is a lab-grown copy of a human immune molecule. Monoclonals could be an effective early treatment for the most serious COVID cases—eventually.
Separate monoclonals are in development by Indiana pharma Eli Lilly and New York rival Regeneron. Eli Lilly paused its trials two weeks ago after independent safety monitors observed an unspecified problem with the testing. It could be months before the FDA can approve either monoclonal for widespread use.
Convalescent plasma is a possible alternative. Operating on a strong hunch this spring and summer, a large number of hospitals drew blood plasma from recovered COVID-19 patients and injected it into the bloodstreams of people with ongoing bad cases of the disease.
The theory was that the antibodies from one person’s plasma might work against someone else’s load of the SARS-CoV-2 virus, hastening their recovery.
Convalescent plasma therapy was popular thanks in large part to a centralized effort by the Mayo Clinic in Minnesota. Working with the FDA, Mayo developed rigorous standards for drawing and administering plasma. Thousands of hospitals and clinics signed up for Mayo’s program. So far, around 86,000 patients have received plasma infusions.
William Hartman, an anesthesiologist at the University of Wisconsin hospital, told The Daily Beast his hospital informs COVID patients of Mayo’s plasma program and gives them the option of enrolling. “Many people are familiar with convalescent plasma at this point and agree to receive it,” he said.
Trump hyped plasma back in August. FDA commissioner Stephen Hahn initially echoed the president’s praise of the unproven therapy before walking back his statement. “The criticism is entirely justified,” Hahn said.
Large-scale trials of convalescent plasma are still underway, and there’s not a lot of hard evidence yet that the plasma actually works, several physicians told The Daily Beast. “Plasma is still controversial given that there is a dearth of controlled trial data,” Yang said. “Many physicians have mostly stopped using it.”
Other unproven therapies have enjoyed bouts of popularity before fading away owing to a lack of positive trial data. Perhaps most notoriously, Trump himself touted hydroxychloroquine as a COVID prophylactic. But multiple trials failed to confirm his claims about the anti-malaria drug. The president also celebrated other dubious “cures” for the coronavirus, including drinking bleach and exposing yourself to ultraviolet light.
Trump didn’t have much to say about some other therapies that quietly rose and fell. This summer, researchers were excited over the possibility that so-called “IL-6 inhibitors” such as Tocilizumab might help calm the hyperactive immune response that’s common in the most severe COVID cases.
But these inhibitors have “fallen off the radar,” Kanthis said. “The data are not as robust as we thought they would be.”
The next hot thing is anti-clotting drugs, several clinicians said. Severe COVID is sometimes associated with dangerous blood clots. “We are still trying to figure out if these patients should be on blood thinners in the form of anticoagulants or antiplatelets,” Sinha Shashank, a cardiologist with the Inova Medical Group in Virginia, told The Daily Beast.
Christopher King, an Inova physician specializing in pulmonary and critical-care medicine, highlighted the anti-clotting drug Fostamatinib, calling it an “exciting potential therapy” for COVID. But trials have just begun. It’s too soon to say whether Fostamatinib is the next Remdesivir … or the next hydroxychloroquine.
“It is important to recognize that the science is still emerging,” Sinha stressed.




